Acute & Chronic Wound Healing Acceleration

On the MULTILINE™ platform, LINLINE accelerates healing of acute surgical wounds and chronic non-healing ulcers using a two-step method: precise Er:YAG ablative sanitation to create a clean, vital wound bed, followed by RecoSMA® field therapy to trigger reparative regeneration—all with minimal collateral trauma and short recovery.
Why this method works
- Clean first, then regenerate. Short-pulse Er:YAG (2.94 μm) removes biofilm, fibrin and necrotic tissue layer-by-layer (≤ ~100 μm/pass) under direct visual control, without deep thermal injury (“blood-dew” endpoint confirms that only non-viable tissue was removed). This creates an optimally prepared bed for healing or secondary closure.
- Deep, non-thermal stimulation. With the SMA module, RecoSMA® delivers thousands of micro-beams (≤ 50 μm; ~10,000/cm²) that launch acoustic waves into the dermis—up to ~6 mm depth—to disrupt pathological structures and activate reparative regeneration (neovascularization, functional tissue replacement) while preserving the epidermal barrier.
- Visible, rapid milestones. After sanitation + RecoSMA®, clinicians commonly observe granulation within 3-5 days and marginal epithelization soon after; pain often decreases within several days.
Indications
- Chronic wounds / ulcers: venous, lymphostatic, arterial, neuro-/diabetic, pressure ulcers, and post-traumatic or post-surgical non-healing wounds.
- Acute surgical complications: infected, dehisced, or necrotic wounds after procedures (e.g., mastopexy, facelift, abdominoplasty, blepharoplasty).
The method may also prepare the wound for secondary sutures or skin grafting sooner, shortening total healing time.
What a session looks like
Step 1 — Ablative sanitation (Er:YAG)
- Goal: remove necrotic tissue, slough, fibrin, biofilm, and reduce microbial load without heating viable layers.
- Technique: short microsecond pulses with visual control until “blood-dew” appears; if residue persists, repeat sanitation. Painless or low-pain when parameters respect tissue thermal relaxation.
Step 2 — RecoSMA® therapy
- Goal: stimulate reparative regeneration in and around the wound; improve microcirculation; counter fibrosis.
- Technique: SMA pass across the wound bed and at least 2-3 cm around the margin; efficacy rises with adequate perilesional coverage.
- Dressings: typically a dry sterile bandage; combine with compression/unloading when indicated (e.g., venous ulcers).
Results you can expect
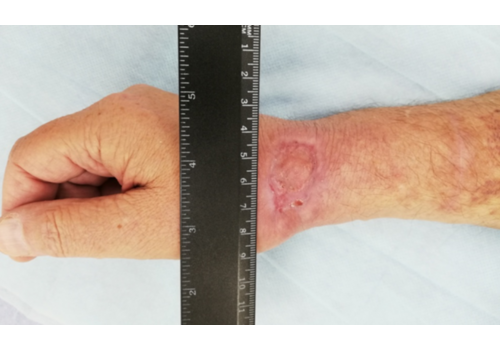
- Chronic ulcers (real-world cases): long-standing venous/lymphatic ulcers healed after courses of Er:YAG sanitation + RecoSMA® (e.g., complete epithelization over weeks to months, often without additional topical drugs).
- Post-op wound dehiscence/infection: daily sanitation + RecoSMA® prepared for secondary sutures in 3–14 days; full closure typically 17–64 days from start, with or without adjunct VAC therapy.
- Aesthetic-surgery wounds: case series report healing in 10–33 days depending on size/severity when combining targeted ablation and RecoSMA®; KTP 540 nm or Nd:YAP/KTP may be added once to normalize microcirculation in select cases.
Course planning
- Chronic ulcer (outpatient): start with more frequent visits (e.g., every 2–3 days → weekly as the wound cleans and granulates) until stable epithelization; number of sessions varies by etiology and off-loading/compression compliance.
- Post-surgical wounds: sanitation daily early on; RecoSMA® 4–6 sessions total depending on response; consider closure once the bed is clean and granulating.
Safety & practical notes
- Er:YAG vs other lasers: choosing 2.94 µm with microsecond pulses enables layered ablation without deep heat—something not achievable with CO₂ or deeper-penetrating IR wavelengths in this indication.
- Treat the cause, too. RecoSMA® accelerates local healing, but etiologic factors (ischemia, venous hypertension, diabetes control, pressure/unloading) must be addressed in parallel. Use compression, off-loading, revascularization, antibiotics, or NPWT as standard of care dictates.
- Pain management: sanitation is usually well tolerated; RecoSMA® can be felt more deeply—reduce pulse frequency rather than energy for comfort.
- Contraindications: uncontrolled systemic infection, untreated ischemia, or inability to comply with compression/off-loading where required. (Clinician judgment prevails.)
Benefits at a glance
For patients
- Faster, cleaner healing with less pain and shorter dressing timelines.
- Lower risk of collateral damage thanks to non-thermal, layer-controlled sanitation.
- Often fewer topical drugs and simpler aftercare once the bed is clean.
For practitioners
- Reproducible endpoints: “blood-dew” for sanitation; granulation/epithelization for progress.
- Versatile workflow: prepares beds for secondary sutures or grafts; integrates with VAC therapy and compression.
- Platform efficiency: runs on MULTILINE™; same RecoSMA® module used across scars and regenerative dermatology.
Key takeaway
By combining micro-controlled Er:YAG sanitation with deep, non-thermal RecoSMA® stimulation, LINLINE provides a structured, platform-based pathway to accelerate healing in acute and chronic wounds—cleaning the bed, jump-starting granulation, and moving patients toward closure faster and more comfortably.
















 06.10.2025
06.10.2025